[译者按:本文根据今年年初生物医学杂志修改关于CAR-NK细胞疗法的述评编译而成,期望对免疫医治有爱好的广阔朋友和(或)肿瘤患者有所协助,不过需求你们耐性点看哈]
1 近10余年来,免疫医治恶性肿瘤的快速开展,如抗-PD-1,抗PD-L1和抗CTLA-4等现已被证明能够治好某些以往底子无法治好晚期恶性肿瘤。
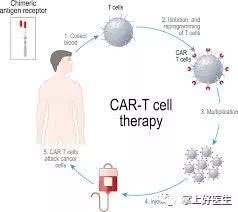
2 2017年美国食品药品管理局(FDA)同意了第一个根据细胞的免疫疗法 嵌合抗原受体(CAR)-T细胞疗法,用于医治难治性B细胞急性淋巴细胞白血病;2018年,FDA又同意了第二个可用于医治B细胞非霍奇金淋巴瘤的CAR-T细胞免疫疗法。
3 2018年,诺贝尔评奖委员会将当年的诺贝尔生理或医学奖颁发给了两位免疫学家 James P Allison and Tasuku Honjo。
4 毫无疑问,前面说到的FDA同意的两种免疫疗法都现已证明了它们在对立癌症方面的重要性,但需求留意的是两种办法都需求有满足的功用正常的T细胞。当医治不含T细胞的所谓“冷肿瘤(cold tumours)”时,或当患者的T细胞简直彻底因“一线医治(指化或放疗)”而消失时,CAR-T医治或许就会因为T-细胞缺少而面对应战。规划捐献的T细胞并扩增它们以取得满足的CAR-T细胞医治是十分耗时的,加之现在可用的CAR-T医治价格也是十分贵重的。此外,CAR-T疗法作为实体瘤(相对于“血液肿瘤“的肿瘤,如肝癌)的医治办法没有完结老练,也即依然有一些作业有待完善。所有这些应战都凸显了寻求其他免疫医治计划的必要性,最近的研讨开展标明天然杀伤(NK)细胞医治是最有期望之星。
5 NK细胞是一种人体取得性免疫必不可少的淋巴细胞之一,它们不需求抗体和首要组织相容性复合物(MHC),就能够辨认“非本身”细胞(或称异体/外源细胞),然后发动快速免疫反响,广泛的细胞毒性和快速的杀灭才能使得NK细胞可望成为癌症免疫疗法的抱负挑选。
6 事实上,早在CAR-T面世之前,研讨人员就企图运用NK细胞来对立癌症,这些测验能够追溯到20世纪80年代后期的临床研讨,但因为技能、后勤和财政等方面的约束,科学家们其时排除了人体血液中本来存在的NK细胞作为令人兴奋和有期望的癌症医治手法。曩昔10多年时刻以来,该范畴现已见证了许多重要的开展。临床前和临床研讨已充沛证明了同种异体NK细胞对各种血液恶性肿瘤和实体瘤的安全性和有用性,其间有些研讨现在还在进行临床试验中。
7 CAR-T细胞医治肿瘤的巨大成功引发了用CAR改进NK细胞的热心,以进步其肿瘤杀伤才能。与CAR-T细胞疗法比较,CAR-NK细胞疗法具有几个特别杰出的长处。首要,与CAR-T细胞不同,CAR-NK细胞保留了经过其天然受体辨认和靶向肿瘤细胞的固有才能,使得经过CAR靶抗原的下调不太或许使肿瘤细胞能够逃逸CAR-NK细胞疗法的进犯;其次,CAR-NK细胞在数天至数周内不会发作克隆扩增或免疫排挤,因而它们不会呈现相同的安全性问题,例如在许多CAR-T临床试验中观察到的细胞因子开释综合征(俗称“细胞因子风暴“)在CAR-NK医治进程简直不存在;终究,NK细胞不需求严厉的HLA匹配,而且缺少引起移植物抗宿主病(GVHD)的或许性,GVHD是CAR-T细胞免疫疗法所面对的严重危险。CAR-NK细胞疗法的这些特色,使得它能够从实验室走向临床,终究成为同种异体的有用细胞免疫疗法。
8 原代NK细胞难以别离,纯化和转导,一般发生扩增不良的异质细胞群。但是,NK细胞系NK-92可在体外简单且无限地扩增,并已在临床中运用,这使其成为发生CAR-NK-92细胞的重要可再生资源。因为一般关于永生细胞系的重视,例如染色体反常和恶性转化的危险,NK-92需求在输注到患者之前进行照耀,这能够按捺NK-92细胞的增殖,一起坚持其彻底细胞毒活性。诱导的多能干细胞(iPSC)能够供给另一种可再生的和或许更好的NK细胞资源。最近在加利福尼亚大学圣地亚哥分校Dan Kaufman小组于2018年6月28日在Cell Stem Cell上宣布的一项临床前研讨探究了这种或许性。研讨人员在人类iPSCs中表达了一种优化的NK特异性CAR构建体,并将这些基因修饰的iPSC分化为功用性NK细胞。他们证明了这些NK-CAR-iPSC-NK细胞在卵巢癌异种移植小鼠模型中明显按捺肿瘤成长。更重要的是,研讨人员比较了iPSC-NK细胞与CAR-T细胞的体内抗肿瘤效能,并发现尽管两种办法都达到了相似的肿瘤杀伤效能,但NK-CAR-iPSC-NK细胞处理的小鼠表现出明显更长的存活率。与CAR-T医治的小鼠比较,没有呈现体重减轻,器官病理学改动或细胞因子水平添加,这标明CAR-NK医治或许比现在的CAR-T医治更安全。这种差异或许使医治患有多剂量CAR-NK细胞的患者变得可行,这或许导致比单剂量更好的临床医治作用,因为用于CAR-T细胞疗法的细胞的有限性和高本钱。
9 尽管CAR-NK疗法在癌症患者中的安全性和有用性需求在更多的临床试验中进一步检测,但令人兴奋的是,咱们现在正在见证一种新的CAR-NK细胞疗法,正在快速赶上CAR-T细胞疗法。CAR-NK好像不太或许替代CAR-T,但它或许是根据细胞的免疫疗法的根本弥补。尽管现在幻想一起用CAR-NK和CAR-T细胞进行联合医治还为时尚早,但最近宣布于临床研讨杂志(2018年9月10日)和细胞(2018年11月29日)的研讨标明,NK细胞或许会发挥作用。在PD-1 / PD-L1阻断免疫疗法中的重要作用以及开释NK细胞和T细胞一起增强抗肿瘤活性。
Natural killer cells for cancer immunotherapy: a new CAR is catching up (EBioMedicine. 2019 Jan; 39: 1–2.)
Immunotherapy has revolutionised cancer treatment. Since the approval of ipilimumab (an anti-cytotoxic T lymphocyte antigen [CTLA]-4 monoclonal antibody) in 2011 for the treatment of patients with malignant melanoma, immune checkpoint inhibitors such as anti-PD-1, anti-PD-L1, and anti-CTLA-4 have demonstrated their power in the clinic to treat previously untreatable terminal tumours. These success stories finally led to James P Allison and Tasuku Honjo winning the Nobel Prize in Physiology or Medicine in 2018. The US Food and Drug Administration (FDA) approved the first cell-based immunotherapy, chimeric antigen receptor (CAR)-T cell therapy, for the treatment of refractory B-cell acute lymphoblastic leukaemia in 2017, and the second one for the treatment of B-cell non-Hodgkin lymphoma in 2018.
Undoubtedly both immunotherapy approaches have proved their own importance in fighting cancer, with a caveat: both require sufficient functional, primary T cells. This requirement can be challenging when treating so-called “cold tumours” that do not contain T cells to be unleashed, or when a patient’s T cells are almost entirely wiped out from a first-line therapy. It can be time-consuming to engineer donated T cells and expand them to obtain enough CAR-T cells, and currently available CAR-T treatments are expensive. Moreover, CAR-T therapy still has some way to go as a therapy for solid tumours. All these challenges highlight the need to seek other immunotherapy options, and recent developments have shown natural killer (NK) cell therapy as one of the most promising.
NK cells are a type of lymphoid cell essential for the innate immune system. They recognise “non-self” cells without the need for antibodies and major histocompatibility complex (MHC), executing a rapid immune reaction. The broad cytotoxicity and rapid killing make NK cells ideal for the use in cancer immunotherapy. Indeed, long before the era of CAR-T, researchers had attempted to harness NK cells to fight cancers. These attempts can be tracked back to clinical studies in the late 1980s, but technical, logistical and financial challenges excluded the application of blood NK cells as an exciting and promising cancer therapy at the time. Over the past decade, the field has witnessed numerous important developments. Pre-clinical and clinical studies have demonstrated the safety and efficacy of allogeneic NK cells against various hematological malignancies and solid tumours and several clinical trials are currently ongoing.
The huge success of CAR-T cells generated enthusiasm to genetically modify NK cells with CARs to sharpen their tumour-killing capacity. CAR-NK cells have several advantages over CAR-T cells. First, unlike CAR-T cells, CAR-NK cells retain an intrinsic capacity to recognise and target tumour cells through their native receptors, making the escaping of tumour cells through downregulation of the CAR target antigen less likely. Second, CAR-NK cells do not undergo clonal expansion or immune rejection within days to weeks, and thus they do not present the same safety concerns, such as cytokine release syndrome, observed in many CAR-T clinical trials. Lastly, NK cells do not require strict HLA matching and lack the potential to cause graft-versus-host disease, an important risk imposed by CAR-T cell immunotherapy, which make it possible for CAR-NK cells to be an off-the-shelf allogeneic therapeutic.
Primary NK cells are difficult to isolate, purify, and transduce, often producing a heterogeneous cell population that expands poorly. However, the NK cell line NK-92 can expand easily and indefinitely in vitro and has been used in the clinic, which makes it a great renewable resource to generate CAR-NK-92 cells. Due to the usual concerns regarding immortal cell lines, such as chromosomal abnormalities and the risk of malignant transformation, NK-92 requires irradiation before infusion into patients, which can suppress proliferation of NK-92 cells while maintaining their full cytotoxic activity. Induced pluripotent stem cells (iPSCs) can offer another renewable and potentially better resources of NK cells. A recent pre-clinical study published in Cell Stem Cell on June 28, 2018, from Dan Kaufman’s group at University of California, San Diego (USA) explored this possibility. The researchers expressed an optimised, NK-specific CAR construct in human iPSCs and differentiated these genetically modified iPSCs into functional NK cells. They were able to show that these NK-CAR-iPSC-NK cells significantly inhibited tumour growth in an ovarian cancer xenograft mouse model. More importantly, the authors compared in vivo antitumour efficacy between iPSC-NK cells with CAR-T cells and found that although both approaches achieved similar tumour-killing efficacy, NK-CAR-iPSC-NK cell-treated mice exhibited significantly longer survival and did not suffer from weight loss, organ pathology, or increased cytokine levels compared with CAR-T treated mice, indicating that CAR-NK therapy might be a safer option than current CAR-T therapy. This difference would probably make it feasible to treat patients with multiple doses of CAR-NK cells, which might lead to better clinical outcomes than with a single dose, which is used for CAR-T cell therapy owing to limited availability of cells and high cost.
While CAR-T cells have produced exciting clinical results, studies using CAR-NK cells have been largely pre-clinical until very recently. Right now, there are more than a dozen clinical trials registered on clinicaltrials.gov to test CAR-NK cell therapy in both haematological and solid tumours, including glioblastoma, prostate cancer, and ovarian cancer. China launched several clinical trials targeting multiple tumours in 2016, and results from one phase 1 clinical trial (published in the American Journal of Cancer Research on June 1, 2018) demonstrated the safety of CD33-CAR-NK-92 cells in patients with relapsed and refractory acute myeloid leukaemia. A European trial testing HER2-specific CAR-NK-92 cells in glioblastoma patients was launched last year, with results expected in the next 2 years. Although both the safety and efficacy of CAR-NK therapy in patients with cancer need to be further tested in more clinical trials, it is exciting that we are now witnessing a new CAR, with NK cells behind the wheel, that is rapidly catching up with CAR-T cells. It seems unlikely that CAR-NK would replace CAR-T, but it could be an addition to the armamentarium of cell-based immunotherapy. Although it is early to imagine a combinational treatment with CAR-NK and CAR-T cells, recent studies published in the Journal of Clinical Investigation (Sept 10, 2018) and Cell (Nov 29, 2018) have indicated that NK cells may play an important role in PD-1/PD-L1 blockade immunotherapy and that unleashing both NK cells and T cells simultaneously enhances anti-tumour activity.
Standing at the beginning of 2019, we are enthusiastic. We expect exciting news from CAR-NK therapy clinical trials. We look forward to embracing CAR-NK cells to join our continuing war against cancer in the coming years.
EBioMedicine